



Pneumonia remains one of the most important causes of mortality. In Portugal, it is the first cause of respiratory death, excluding lung cancer. This is a retrospective cohort study designed to seek for explanations, identifying the characteristics of patients and measure the impact of each one of them on the risk of dying from pneumonia. We analyzed demographic and clinical data of all patients (pts) with 18 years or older with pneumonia requiring hospitalization registered on the national health service registry of mainland Portugal over 2015. A total of 36366 patients corresponding to 40696 pneumonia hospital admissions in 2015 were analyzed. Most of the patients were very old (median age 80 years). Hospital mortality for pneumonia was higher among older (30,3% pts>75 years). Pneumococcus is the more frequent bacterial isolate, reaching 41.2% of the isolates of total pneumonia cases. The frequency of pneumococcus decreases with aging; conversely, gram-negative bacteria and staphylococcus increase. Pneumococcus is more frequently identified in the winter, closely related to influenza outbreaks. Gram-negative bacteria are more prevalent during the summer months. Diabetes, obesity, COPD, and tobacco smoking are not associated with an increased risk of dying from pneumonia. Patients older than 75 years; living in a senior house; or with chronic renal disease, lung cancer, metastatic disease, mobility impairment, cachexia, dementia, cerebrovascular disease, and ischemic heart disease are at greater risk of dying from pneumonia. Comorbidities contribute decisively to the risk of dying from pneumonia in the hospital, regardless of their type or origin.
Pneumonia has always been recognized as a terrifying disease. William Osler1 in the nineteenth century made multiple descriptions of its different forms of presentation and their relationship with frail, vulnerable, and elderly people.1 Despite medical science, better health-care access, specialized units, sophisticated life-support systems, and even extracorporeal membrane oxygenation (ECMO), year after year, pneumonia mortality rates reach 30% of all respiratory causes of death in the Organization for Economic Cooperation and Development (OECD) countries report.2 According to the last OECD report, Portugal had one of the highest rates of pneumonia mortality.2 The figures on pneumonia occurrence and their distribution in the community (CAP) are almost impossible to determine accurately. Studying hospital admissions for moderate to severe pneumonias has been one way to understand the characteristics and the impact of this disease,3,4 at least the most severe cases. In Portugal, pneumonia is certainly one of the main causes of death, representing 43.9% of all respiratory mortality, excluding lung cancer,5 in 2015. This study was designed to seek explanations for these observations. We intend to analyze occurrence patterns, the distribution and the clinical characteristics of the patients with moderate and severe pneumonias requiring hospital admission to identify the main determinants of their morbimortality.
ObjectiveThis study aims to evaluate the demographic distribution and clinical patterns associated with patients with pneumonia requiring hospitalization and their impact on mortality. Using all pneumonia cases admitted during 2015, we will create a risk model generating outcome estimates on the risk of dying for each individual patient.
Patients and methodsThis is a joint project of the Portuguese Society of Pulmonology and the Priority Health Program for Respiratory Diseases of the Portuguese General Directorate of Health.
In this study, we retrospectively analyzed all patients requiring hospitalization for pneumonia in the National Health Service (NHS) hospitals in mainland Portugal in 2015. The Central Administration of the Portuguese Health System of the Ministry of Health (ACSS) keeps administrative, demographic, and clinical data of all admissions of NHS hospitals that cover the whole Portuguese resident population. The entirely anonymized patients’ data, encoded from medical records by specialized codifiers, using the International Classification of Diseases, Ninth Revision Clinical Modification (ICD-9-CM),6 was the data source for this study.
To make the study more patient-driven, a code number from each patient was generated, maintaining absolute anonymization, allowing us identify if a particular database entry, was a primary case or a readmission. The age, gender, geographical location of residence and hospital where the admission occurred, date of hospitalization up to the first five registered diagnoses by hospital admission, procedures, etiologic microbial information, previous surgery or traumatic event, readmission event, time of readmission, and outcome were the primary data we retrieved from the database. This database included up to 20 entries for diagnosis and procedures. We decided to include the first five registered diagnoses because the majority of the admissions had, at least, five entries for diagnosis.
To make diagnostic information usable, we developed a decision tree, creating diagnostic groups built from the diagnostic codes of the ICD-9-CM registered at each hospitalization (supplementary material). The diagnostic groups were constructed in a way that could easily be classified as comorbidities (diabetes, chronic renal failure, dementia, cachexia, cancer metastatic disease, obesity, alcohol/tobacco, etc.) or complications of the pneumonia if they were being classified as consequences of the disease (sepsis, respiratory failure, shock, empyema, acute renal failure, acid-base or hydroelectrolytic disturbances, etc.). After this classification procedure (supplementary material), the patients’ characteristics (age group, gender, diabetes, asthma, COPD, cerebrovascular-disease sequels, dementia, mobility impairment of any cause, cachexia, ischemic heart disease, chronic renal failure, cancer of any site, metastatic cancer, lung cancer, tobacco smoking, obesity, living in a senior house, length of patient stay, airway aspiration, sepsis, sepsis and shock) and microbiologic data were analyzed.
Inclusion criteriaPatients aged 18 years or older admitted to hospital with a discharge primary diagnosis of pneumonia (ICD-9-CM 480–486, 487.0) or patients hospitalized with primary diagnosis of sepsis (ICD-9-CM 038-0389) if the diagnosis of pneumonia was, at least, present in the second of the five analyzed discharge diagnosis, were included.
Exclusion criteriaPatients younger than 18 years old or hospitalized with a discharge primary diagnosis other than pneumonia or a primary diagnosis of sepsis and other than pneumonia in the second diagnosis were excluded.
Statistical analysisThe clinical and demographic variables (see Table 1) were transformed into indicator variables and coded as0 if the characteristic was absent and 1if present. The median and age-group intervals presented age. The generated age-group variable “age 75” was dichotomous—1 if the patient was 75 or older and 0 if this condition was not met. Clinical variables (diabetes, chronic renal disease, shock, COPD, lung cancer, obesity, etc.) were coded 1 if present and 0 if absent. The outcome of the disease was coded 1 if death occurred and 0 if otherwise and the patient recovered from the disease. The interaction of all these variables and disease outcome was expressed as odds ratios (ORs). Some of them were also displayed as forest plots. A logistic regression was created to adjust the influence between the patient characteristics and the outcome.7 The individual patient outcome estimates could be obtained by getting the sum of the products of the coefficient of each independent variable (β1-n) included in the logistic model (Fig. 2) and their code (X1-n)—1 if a particular characteristic was present and 0 if absent—and replacing this in the formula 1/1+e-(Constant-∑(β1X1+ β2X2+… βnXn))obtain the individual probability of the risk of dying from pneumonia in a hospital. We used STATA Statistical Data Analysis 9.08 and BiostatXL MIX 2.0 (available at: http://www.meta-analysis-made-easy.com) to compute all these estimates.9
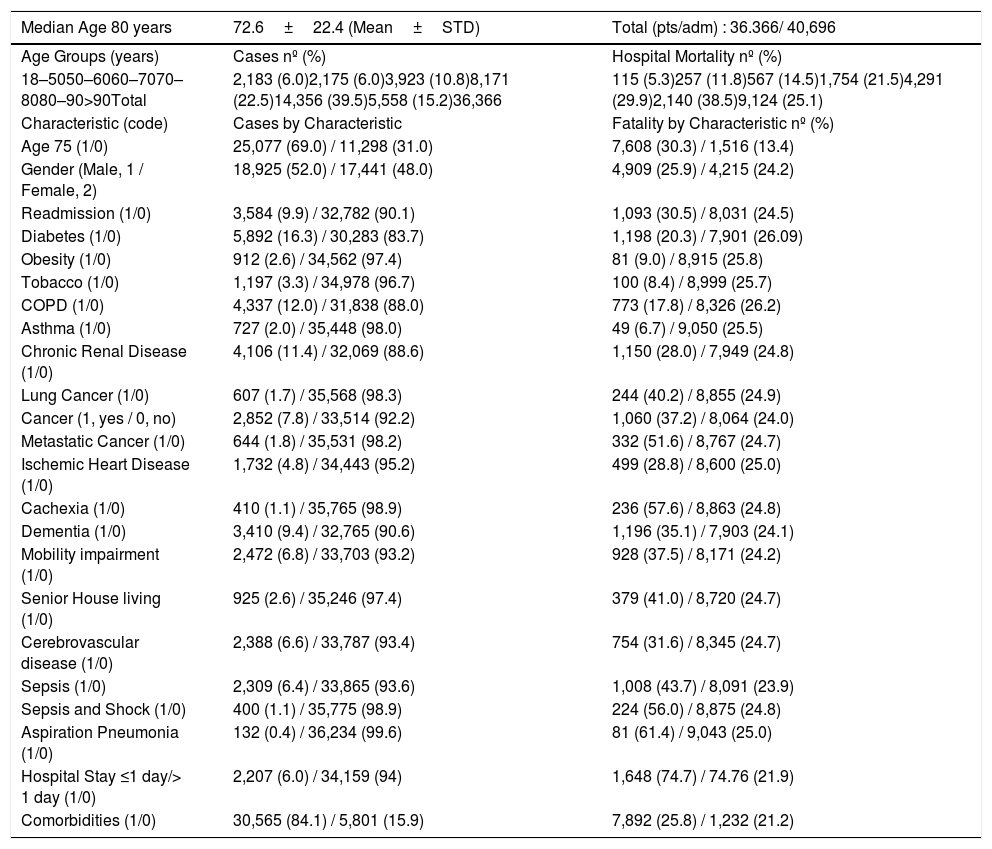
Patients & Characteristics & Case Fatalities.
| Median Age 80 years | 72.6±22.4 (Mean±STD) | Total (pts/adm) : 36.366/ 40,696 |
|---|---|---|
| Age Groups (years) | Cases nº (%) | Hospital Mortality nº (%) |
| 18–5050–6060–7070–8080–90>90Total | 2,183 (6.0)2,175 (6.0)3,923 (10.8)8,171 (22.5)14,356 (39.5)5,558 (15.2)36,366 | 115 (5.3)257 (11.8)567 (14.5)1,754 (21.5)4,291 (29.9)2,140 (38.5)9,124 (25.1) |
| Characteristic (code) | Cases by Characteristic | Fatality by Characteristic nº (%) |
| Age 75 (1/0) | 25,077 (69.0) / 11,298 (31.0) | 7,608 (30.3) / 1,516 (13.4) |
| Gender (Male, 1 / Female, 2) | 18,925 (52.0) / 17,441 (48.0) | 4,909 (25.9) / 4,215 (24.2) |
| Readmission (1/0) | 3,584 (9.9) / 32,782 (90.1) | 1,093 (30.5) / 8,031 (24.5) |
| Diabetes (1/0) | 5,892 (16.3) / 30,283 (83.7) | 1,198 (20.3) / 7,901 (26.09) |
| Obesity (1/0) | 912 (2.6) / 34,562 (97.4) | 81 (9.0) / 8,915 (25.8) |
| Tobacco (1/0) | 1,197 (3.3) / 34,978 (96.7) | 100 (8.4) / 8,999 (25.7) |
| COPD (1/0) | 4,337 (12.0) / 31,838 (88.0) | 773 (17.8) / 8,326 (26.2) |
| Asthma (1/0) | 727 (2.0) / 35,448 (98.0) | 49 (6.7) / 9,050 (25.5) |
| Chronic Renal Disease (1/0) | 4,106 (11.4) / 32,069 (88.6) | 1,150 (28.0) / 7,949 (24.8) |
| Lung Cancer (1/0) | 607 (1.7) / 35,568 (98.3) | 244 (40.2) / 8,855 (24.9) |
| Cancer (1, yes / 0, no) | 2,852 (7.8) / 33,514 (92.2) | 1,060 (37.2) / 8,064 (24.0) |
| Metastatic Cancer (1/0) | 644 (1.8) / 35,531 (98.2) | 332 (51.6) / 8,767 (24.7) |
| Ischemic Heart Disease (1/0) | 1,732 (4.8) / 34,443 (95.2) | 499 (28.8) / 8,600 (25.0) |
| Cachexia (1/0) | 410 (1.1) / 35,765 (98.9) | 236 (57.6) / 8,863 (24.8) |
| Dementia (1/0) | 3,410 (9.4) / 32,765 (90.6) | 1,196 (35.1) / 7,903 (24.1) |
| Mobility impairment (1/0) | 2,472 (6.8) / 33,703 (93.2) | 928 (37.5) / 8,171 (24.2) |
| Senior House living (1/0) | 925 (2.6) / 35,246 (97.4) | 379 (41.0) / 8,720 (24.7) |
| Cerebrovascular disease (1/0) | 2,388 (6.6) / 33,787 (93.4) | 754 (31.6) / 8,345 (24.7) |
| Sepsis (1/0) | 2,309 (6.4) / 33,865 (93.6) | 1,008 (43.7) / 8,091 (23.9) |
| Sepsis and Shock (1/0) | 400 (1.1) / 35,775 (98.9) | 224 (56.0) / 8,875 (24.8) |
| Aspiration Pneumonia (1/0) | 132 (0.4) / 36,234 (99.6) | 81 (61.4) / 9,043 (25.0) |
| Hospital Stay ≤1 day/> 1 day (1/0) | 2,207 (6.0) / 34,159 (94) | 1,648 (74.7) / 74.76 (21.9) |
| Comorbidities (1/0) | 30,565 (84.1) / 5,801 (15.9) | 7,892 (25.8) / 1,232 (21.2) |
Coded 1 if the characteristic is present, 0 if absent; pts (patients)/adm (admissions).
A total of 36,366 patients corresponding to 40,696 pneumonia hospital admissions in 2015 (Table 1) were evaluable. Hospital mortality (case-fatality) was higher among patients with multiple admissions (30.6% vs. 24.5%).
Most of the patients were hospitalized from 1 to 15 days. Most of the patients (see Table1) were very old, 18,655 (47.1%) aged 80 or older. Hospital mortality increased sharply after the 60s, reaching 38.5% after the 90s.
Most of the patients admitted to hospital for pneumonia were male 18,925 (52%). Diabetes, COPD, and chronic renal disease (CRD) were present in 5892 (16.3%), 4337 (12%), and 4106 (11.4%) of the patients, respectively (Table 1). Cancer of any site was present in 2852 (7.8%) patients, including 607 (1.7%) with lung cancer and 644 (1.8%) with metastatic disease. Cardiac ischemic disease was an important comorbidity identified in 1732 (4.8%) patients. Dementia, serious mobility impairment, cerebrovascular disease, cachexia, and living in senior housing were identified in 3410 (9.4%), 2472 (6.8%), 2388 (6.6%), 410 (1.1%), and 925 (2.6%), respectively, of the pneumonia patients.
Only in 3220 (8.9%) of the pneumonia admissions was it possible to establish the etiology of the pneumonia (supplementary material). Pneumococcus was the microbiologic agent most frequently identified. Other bacteria such as miscellaneous gram-negative and multiresistant Staphylococcus aureus were also relevant isolates identified in the patients with pneumonia requiring hospitalization.
Most pneumonia admissions happened during the colder months, closely related to peak rates of influenza. However, the highest pneumonia hospital mortality rates occurred during the summer from July to September (supplementary material).
The distribution of microbiological isolates showed us the predominance of Pneumococcus during the entire year (supplementary material), representing more than 40% of all virus and bacteria identifications. The microbiologic identifications had different distributions throughout the months of the year (supplementary material). There is a proportional increase of the identification rate of Staphylococcus and gram-negative bacteria species, from July to September (supplementary material). During winter (December, January, and February), most bacteria isolates were Pneumococcus. The microbiology seemed to be related to the age of the patients (supplementary material). Pneumococcus and atypical bacteria were more frequently identified in younger age groups. Conversely, among the elderly, apart from Pneumococcus, Staphylococcus, including multiresistant Staphylococcus aureus (MRSA) and miscellaneous gram-bacteria (supplementary material), plays the most important role. There is a clear downward trend of the frequency of pneumococcal isolates from the 50s (supplementary material). The atypical bacteria were most frequently identified in the 18–50 age group, decreasing from there on. Older age groups were more prone to get pneumonia caused by gram-negative and Staphylococcus bacteria and be admitted to the hospital.
From all patients’ characteristics, we selected the most frequent to evaluate their impact on pneumonia hospital mortality. These characteristics were classified into four groups: patient general condition, comorbidities, microbiology, and complications. We found a significant statistical association (Fig. 1) between the risk of dying and the condition of several of these patients, comorbidities, microbiology, or complications. Patients older than 75 years old; living in senior housing; with chronic renal disease, lung cancer, metastatic disease, mobility impairment, cachexia, dementia, cerebrovascular disease (CVD), or ischemic heart disease (IHD) are at greater risk of dying from pneumonia. Conversely, gender, obesity, tobacco consumption, diabetes, and COPD were not associated with an increased risk of dying for pneumonia patients admitted to hospital. The MRSA, Pseudomonas, aspiration pneumonia, shock, sepsis, hospital readmissions, and one day or even less of hospitalization are, on the contrary, significantly associated with an increased risk of dying from pneumonia. It is noteworthy that the identification of a Pneumococcus is associated with a lower risk of dying from pneumonia (Fig. 1).
![Pneumonia Hospital Mortality – Sub-group analysis. [OR (odds ratio), CRD (chronic renal disease), CVD (cerebrovascular disease), IHD (ischemic heart disease), MRSA (multiresistant Staphylococcus aureus), E. coli (Escherichia coli); hospital ≤1/>1 (days of hospital stay)]](https://static.elsevier.es/multimedia/25310437/0000002600000003/v1_202005111106/S2531043719302053/v1_202005111106/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w94UphxYc+GPca8Z7OggvdfJaI9Nqk/wRF1/+NWFHb4fNmbzo7o4+FCBjEme9N3mE3bTUWDaXJE7QOR9IbzHlTqO1PidqiIsVPVJZ+ymjDWBfAZzvP83PcsAPHVf+kylTXaydi0H/U7FFF5TfMADl2f3pjlhKjAH14sairKiaGoS7b0oXHCHft8wloLwFvckrlZouF2zs7UVW3Zohn/voU0shaA/12oHlNqcxx2LmKruatguecwBvPmDrjDx7hyfQvvBVJfL3ZV1er2CCbN0bhUk= "Pneumonia Hospital Mortality – Sub-group analysis. [OR (odds ratio), CRD (chronic renal disease), CVD (cerebrovascular disease), IHD (ischemic heart disease), MRSA (multiresistant Staphylococcus aureus), E. coli (Escherichia coli); hospital ≤1/>1 (days of hospital stay)]")
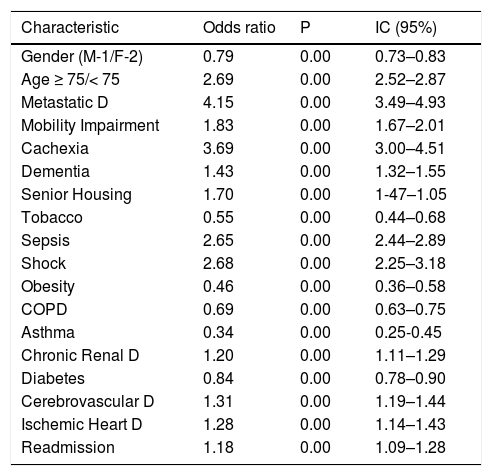
After adjusting for the risk of death from the patients’ characteristics, we identified that individuals in the age group over, or equal to 75 years old, who were living in senior housing, or had previous cerebrovascular disease, cardiac or renal chronic disease, dementia, cachexia, mobility impair, neoplastic metastatic disease, or upfront sepsis were significantly associated with an increased risk of dying from pneumonia in the hospital (see Table 2).
Pneumonia Hospital Mortality, Adjusted Risk Factors (nº cases - 35,470).
| Characteristic | Odds ratio | P | IC (95%) |
|---|---|---|---|
| Gender (M-1/F-2) | 0.79 | 0.00 | 0.73–0.83 |
| Age ≥ 75/< 75 | 2.69 | 0.00 | 2.52–2.87 |
| Metastatic D | 4.15 | 0.00 | 3.49–4.93 |
| Mobility Impairment | 1.83 | 0.00 | 1.67–2.01 |
| Cachexia | 3.69 | 0.00 | 3.00–4.51 |
| Dementia | 1.43 | 0.00 | 1.32–1.55 |
| Senior Housing | 1.70 | 0.00 | 1-47–1.05 |
| Tobacco | 0.55 | 0.00 | 0.44–0.68 |
| Sepsis | 2.65 | 0.00 | 2.44–2.89 |
| Shock | 2.68 | 0.00 | 2.25–3.18 |
| Obesity | 0.46 | 0.00 | 0.36–0.58 |
| COPD | 0.69 | 0.00 | 0.63–0.75 |
| Asthma | 0.34 | 0.00 | 0.25-0.45 |
| Chronic Renal D | 1.20 | 0.00 | 1.11–1.29 |
| Diabetes | 0.84 | 0.00 | 0.78–0.90 |
| Cerebrovascular D | 1.31 | 0.00 | 1.19–1.44 |
| Ischemic Heart D | 1.28 | 0.00 | 1.14–1.43 |
| Readmission | 1.18 | 0.00 | 1.09–1.28 |
Using these estimates it was possible to compute a predictive model for patients with pneumonia which required hospital admission, quantifying their individual risk of dying, from this disease (Fig. 2).
Discussion
The main findings of this study led us to understand that an overwhelming majority of patients dying from pneumonia had one or more severe chronic diseases, which certainly contributed to the outcome. According to a recent publication of health data in the OECD, the life expectancy at age 65 in Portugal is 17 years for males and 23 for females.2 However, more than half of that time is spent struggling with some sort of disease.2 Despite treatment conditions and full access to health services by the Portuguese population, we verified, year after year, an increase in mortality due to pneumonia in Portugal.2 We are absolutely convinced that this entire chronic disease burden could affect the pneumonia figures, not only in incidence but also in mortality. This study’s main motivation was to look for explanations of such a situation and try to prepare future strategies to minimize the impact of this disease on mortality. Portugal has a centralized system of registration for all hospital admissions involving all NHS hospitals. Beyond the administrative data, we have access to fully anonymized clinical data. Usually, these data are not patient-driven; only admission episodes are available for analysis. However, generating a code number from the real patient identification was possible, maintaining total patient anonymization and allowing us to identify the readmissions and, therefore, to study patients instead of admissions.
This study has several limitations. This is a retrospective database analysis, so there is the possibility of information bias and misclassification. Adjustments were made for demographics, clinic and microbiologic variables. However, some important patient characteristics (pneumonia severity PSI or CURB65 classification, mechanical ventilation-vasopressors; vaccinations; empiric antibiotics; suitability of antibiotic choice with bacterial isolates; co-infections; specimen isolates and bacteremia), could not be analyzed because they were not present in NHS database. Despite all these limitations, this study evaluates a large number of patients, representing all the NHS patients from an entire country, hospitalized for severe pneumonia, over the course of one year.
We studied 36,366 patients which corresponded to 40,696 hospital admissions in 2015. The main targets of this study were patient characteristics, particularly comorbidities and their influence on the outcome. The great majority of the patients with severe pneumonia were elderly, in total 30,565 (84.1%) (see Table 1), and had at least one chronic long-standing disease. Similar to other studies,10,11 the elderly were more susceptible to getting sick with pneumonia and being hospitalized.
Most of the pneumonias occurred during winter; however, the deadliest happened from July to September. Host factors have been increasingly considered as decisive for the outcome of the patients with severe pneumonia.11,12 In our study, advanced age, dementia, mobility impairment, metastatic cancer, and living in senior housing were some of the more important prehospitalization conditions and comorbidities of the patients hospitalized in 2015 with severe pneumonia in Portugal. As in other studies,13–17 these patients’ characteristics have been shown to be a determinant for the increased risk of dying from pneumonia. Pneumonia after viral infections18 is a common occurrence, this is explained, although not completely understood, by association with the host biological factors,19 disruption of the mucosal barrier, and ciliary malfunction caused by a previous viral infection impairing the viral or bacterial clearance, facilitating bacterial colonization and, subsequently, the pneumonia.18,19
We identified bacterial isolates in 3220 (8.9%) of our patients. The distribution of the microbiological isolates by age groups had shown that among the patients hospitalized for pneumonia, the frequency of pneumococcus decreased sharply with age; younger patients had more frequent pneumococcus isolates than older patients. This observation could explain the apparent “protective effect” of the association between pneumonia with pneumococcus identification and the lower risk of death.
A plausible explanation of this observation could be that pneumococcal pneumonia is in our series more frequent in younger patients and, therefore, less likely to have major comorbidities that can increase the risk of dying. The distribution of bacterial isolates throughout the year shows that during summer, there is proportionally, more frequent identification of gram-negatives and staphylococcus than in other months. This situation can be related to the excess mortality observed during those months. Regardless of the type, severe pneumonia determining hospitalization, the risk of dying seems to be more related to the comorbidities than with the etiology. On the contrary, probably the general condition of the patients and their susceptibilities also deeply influence the microbial agent. Diabetes, COPD, obesity, and tobacco smoking are usually related to pneumonia and the risk of hospitalization.20,21 However, in our study, they are negatively associated with the risk of dying from pneumonia.
Chronic renal failure and ischemic heart disease are two important risk factors of pneumonia death. We observed from our data the association of the risk of death and the length of hospital stay. The risk of death for pneumonia was higher for short stays, decreasing afterward. This observation led us to consider that a significant number of patients might have been diagnosed and started the treatment later in the course of the disease. If we examine the age and the comorbidities of most of the patients and the possibility of many of them living alone, the latter hypothesis can be convincing.
ConclusionRegardless of the importance of the etiology and the treatment, the characteristics of the host might be key to explaining the high mortality due to pneumonia we found in our data. Elderly patients and the high proportion of major comorbidities such as dementia, cachexia, severe mobility impairment, metastatic cancer, chronic renal disease, ischemic heart disease, cerebrovascular disease, sepsis on hospital admission and senior house living, are independent risk factors of dying from pneumonia in a hospital
Authors contributionConceptualization, Methodology, Formal analysis: Venceslau Hespanhol
Conceptualization: Cristina Bárbara
Financial support: no financial support involved
Manuscript writing: All authors
Final approval of manuscript: All authors
Conflicts of interestAuthors have no conflicts of interest to declare, regarding the present work
The authors gratefully acknowledged Professor Fernando Araujo, Secretary of State of Health of Portuguese Government and Dr. Ricardo Mestre, Central Administration of Health System (ACSS) by the encouragement and assistance in accessing national databases, making this work possible.
The following are Supplementary data to this article:


