



Poland Syndrome is a rare congenital deformity which mainly occurs sporadically but occasional familial cases have been reported.1 It is characterized by unilateral absence of pectoralis muscle, typically in association with other deformities of the ipsilateral chest wall and/or upper limbs.1 According to recent classifications, the pectoralis muscle anomaly alone is enough to establish diagnosis.2 It predominantly affects the right hemithorax (67-75%), with rare bilateral cases described.(1) The most commonly accepted causal mechanism is related to disruption of blood supply through the subclavian artery during embryogenesis.3 Incidence varies from 1/70000 to 1/100000 live births, with a male to female ratio of 2-3 to 1.(1) Due to mild or even non-existent functional impairment, the condition is thought to be under-reported and underdiagnosed. Surgical correction is recommended in cases of significant functional or aesthetic impairment.4
We report the case of a 19 year-old male, admitted to the emergency room presenting with left-sided chest pain 24hours after onset. He had no other complaints and there was no precipitating event, such as, trauma or infection.The patient was a non-smoker; with no relevant personal or family past medical history.
Physical examination showed the patient to be tachycardic and slightly polypneic. Thoracic inspection showed hypoplasia of the left thoracic wall due to the underdevelopment of the left pectoralis muscle and decreased chest expansion. No other structural abnormalities were observed on the affected side of the torso.
Also on the left hemithorax, there was hyperresonance to percussion and absent breath sounds on ausculation.
Chest x-ray showed a large left lung pneumothorax; a chest tube was successfully placed with clinical improvement and total lung expansion. Thoracic computer tomography (Figures 1 and 2) revealed hypoplasia of the major pectoralis muscle confirming the diagnosis of Poland Syndrome and ruled out other abnormalities. There was full resolution of the pneumothorax and the chest tube was removed after four days.


The definition of Poland Syndrome includes variable musculoskeletal deformities in multiple musculoskeletal structures, typically ipsilateral to the pectoralis major muscle hypoplasia.1 As it is a rare, heterogeneous condition, the documentation of clinical cases and case series is of particular relevance for better understanding of its causes and physiopathology.
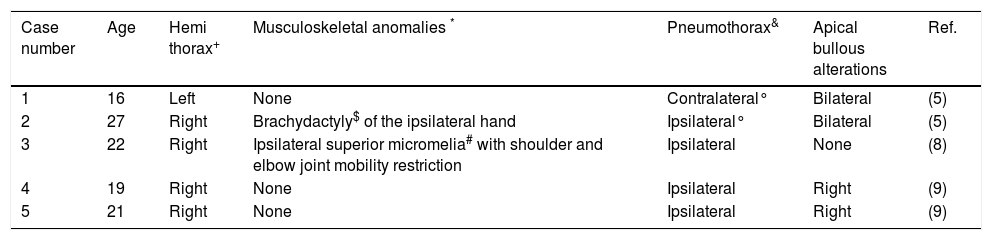
The case here presented of Poland syndrome and pneumothorax reinforces the hypothesis of an association between the two clinical entities. We carried out a systematic review on Pubmed and Embase databases; the results are summarised in Table 1. We identified five cases, all male patients, aged between 16 and 27 years. As well as the case described, there was one other which presented with a left-sided deformity, and three isolated pectoralis major muscle anomalies. Only in one case was the pneumothorax contralateral to the muscle hypoplasia; in four patients parenchymal bullae were found. The prevailing theory about the pathophysiology of this association refers to changes in the blood supply through the brachial arch during embryogenesis.3,5 Disruption at this level potentially affects the development of the lungs and pleura, increasing the risk of spontaneous primary pneumothorax. Cigarette smoking as an additional risk factor for pneumothorax should be considered, although no information about smoking habits has been included in previous case reports. Management approaches for primary spontaneous pneumothorax vary widely between institutions. The recommendations of the British Thoracic Society favour a conservative approach preferring aspiration to thoracostomy,6 however it is recognized that this approach is often ineffective and many medical institutions do not follow these recommendations.7 In the case described, a 24F chest tube was chosen based on availability and experience in our emergency services. The first episodes of cases 1 and 2,5 as well as case 3,8 were also managed by thoracostomy. The recurrent nature of cases 1 and 25 and the existence of bullous parenchymal changes in cases 4 and 59 led to a decision for surgical treatment. We can also draw attention to the fact that there are no specific recommendations for the treatment of pneumothorax in a patient with Poland Syndrome. There was a positive clinical outcome in all the cases reported, including this one.
Main characteristics of previous described cases associating Poland syndrome and pneumothorax. All patients were male.
| Case number | Age | Hemi thorax+ | Musculoskeletal anomalies * | Pneumothorax& | Apical bullous alterations | Ref. |
|---|---|---|---|---|---|---|
| 1 | 16 | Left | None | Contralateral° | Bilateral | (5) |
| 2 | 27 | Right | Brachydactyly$ of the ipsilateral hand | Ipsilateral° | Bilateral | (5) |
| 3 | 22 | Right | Ipsilateral superior micromelia# with shoulder and elbow joint mobility restriction | Ipsilateral | None | (8) |
| 4 | 19 | Right | None | Ipsilateral | Right | (9) |
| 5 | 21 | Right | None | Ipsilateral | Right | (9) |
+ Location of pectoralis muscle deformity; * Additional musculoskeletal deformities; & Location in relation to the pectoralis muscle deformity; $ Shortening of fingers; # Limb shortening;° Recurrent pneumothorax.
This case supports the theory that the morphological alterations observed in Poland syndrome can extend to the pleural and pulmonary parenchyma and that therefore this population may benefit from greater clinical surveillance.
The possible hypothesized association between these two clinical entities is dependent on the reporting and analysis of more cases. Also, longitudinal epidemiological studies may be useful.
DisclosureThe authors report no financial support, off-label or investigational drug use.
Conflicts of interestThe authors have no conflict of interest to declare.


