

Little is known about the relationship between the COVID-19 and tuberculosis (TB). The aim of this study is to describe a group of patients who died with TB (active disease or sequelae) and COVID-19 in two cohorts.
Data from 49 consecutive cases in 8 countries (cohort A) and 20 hospitalised patients with TB and COVID-19 (cohort B) were analysed and patients who died were described. Demographic and clinical variables were retrospectively collected, including co-morbidities and risk factors for TB and COVID-19 mortality.
Overall, 8 out of 69 (11.6%) patients died, 7 from cohort A (14.3%) and one from cohort B (5%).
Out of 69 patients 43 were migrants, 26/49 (53.1%) in cohort A and 17/20 (85.0%) in cohort B.
Migrants: (1) were younger than natives; in cohort A the median (IQR) age was 40 (27–49) VS. 66 (46–70) years, whereas in cohort B 37 (27–46) VS. 48 (47–60) years; (2) had a lower mortality rate than natives (1/43, 2.3% versus 7/26, 26.9%; p-value: 0.002); (3) had fewer co-morbidities than natives (23/43, 53.5% versus 5/26–19.2%) natives; p-value: 0.005).
The study findings show that: (1) mortality is likely to occur in elderly patients with co-morbidities; (2) TB might not be a major determinant of mortality and (3) migrants had lower mortality, probably because of their younger age and lower number of co-morbidities. However, in settings where advanced forms of TB frequently occur and are caused by drug-resistant strains of M. tuberculosis, higher mortality rates can be expected in young individuals.
The COVID-19 pandemic caused by the SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) is causing a debate on preventive, diagnostic, and therapeutic strategies among scientists, clinicians, and public health experts.1–3
The current scientific evidence suggests that individuals with the disease are infectious, SARS-CoV-2 rapidly spreads within the community because of the lack of herd immunity,4,5 it has high case-fatality rate among elderly and patients with co-morbidities and can stretch unprepared healthcare systems causing rapid collapse of intensive care units (ICU).1,6
Patients with COVID-19 may complain of cough, fever, tiredness, dyspnoea, and other signs and symptoms1–3 similar to those of tuberculosis (TB) and of other respiratory infections.7
Little is known about the relationship between the COVID-19 and TB. Data from 49 cases (cohort A) reported elsewhere7 show that COVID-19 can occur before, simultaneously, or after the diagnosis of TB. Furthermore, additional information from 20 hospitalised patients with TB and COVID-19 (cohort B) is available (Stochino C. et al, unpublished data).
The aim of this study is to describe for the first time a group of patients who died with TB (active disease or sequelae) and COVID-19 in the cohorts A and B.
Patients and methodsData of both cohorts were combined to assess the mortality. Cohort A included 49 patients with TB and COVID-19 from 26 centres in Belgium, Brazil, France, Italy, Russia, Singapore, Spain, and Switzerland,7 whereas cohort B included 20 cases admitted to a single reference hospital located in Northern Italy.
Both cohorts belong to nested studies of the Global Tuberculosis Network (GTN) large observational project monitoring adverse reactions to anti-TB drugs for which the coordinating centre in Tradate (Italy) has the ethical approval (and other participating centres according to the respective national regulations).7–9
All consecutive cases with a diagnosis of TB (at any time in the past, so as to include patients with TB sequelae, which may be a risk factor for mortality) and COVID-19 from cohorts A and B were included.
Demographic and clinical variables were retrospectively collected, including co-morbidities and risk factors for TB and COVID-19 mortality.
TB patients were microbiologically confirmed (Table 1), whereas SARS-CoV-2 infection was confirmed by molecular biology. The first COVID-19 diagnosis was made on March 12th, 2020; data were updated as of May 5th, 2020.
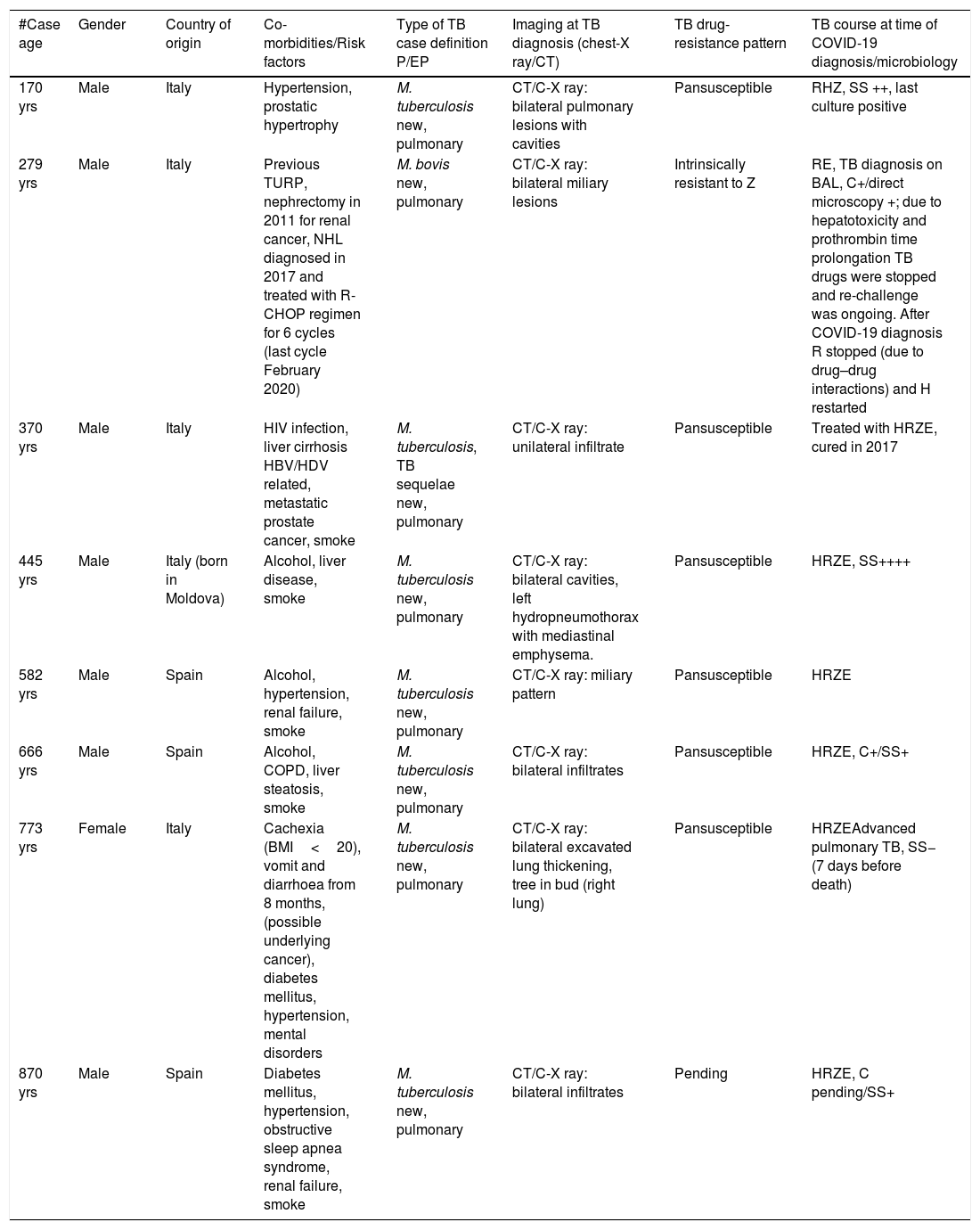
Information on tuberculosis in 8 patients with COVID-19 who died.
| #Case age | Gender | Country of origin | Co-morbidities/Risk factors | Type of TB case definition P/EP | Imaging at TB diagnosis (chest-X ray/CT) | TB drug-resistance pattern | TB course at time of COVID-19 diagnosis/microbiology |
|---|---|---|---|---|---|---|---|
| 170 yrs | Male | Italy | Hypertension, prostatic hypertrophy | M. tuberculosis new, pulmonary | CT/C-X ray: bilateral pulmonary lesions with cavities | Pansusceptible | RHZ, SS ++, last culture positive |
| 279 yrs | Male | Italy | Previous TURP, nephrectomy in 2011 for renal cancer, NHL diagnosed in 2017 and treated with R-CHOP regimen for 6 cycles (last cycle February 2020) | M. bovis new, pulmonary | CT/C-X ray: bilateral miliary lesions | Intrinsically resistant to Z | RE, TB diagnosis on BAL, C+/direct microscopy +; due to hepatotoxicity and prothrombin time prolongation TB drugs were stopped and re-challenge was ongoing. After COVID-19 diagnosis R stopped (due to drug–drug interactions) and H restarted |
| 370 yrs | Male | Italy | HIV infection, liver cirrhosis HBV/HDV related, metastatic prostate cancer, smoke | M. tuberculosis, TB sequelae new, pulmonary | CT/C-X ray: unilateral infiltrate | Pansusceptible | Treated with HRZE, cured in 2017 |
| 445 yrs | Male | Italy (born in Moldova) | Alcohol, liver disease, smoke | M. tuberculosis new, pulmonary | CT/C-X ray: bilateral cavities, left hydropneumothorax with mediastinal emphysema. | Pansusceptible | HRZE, SS++++ |
| 582 yrs | Male | Spain | Alcohol, hypertension, renal failure, smoke | M. tuberculosis new, pulmonary | CT/C-X ray: miliary pattern | Pansusceptible | HRZE |
| 666 yrs | Male | Spain | Alcohol, COPD, liver steatosis, smoke | M. tuberculosis new, pulmonary | CT/C-X ray: bilateral infiltrates | Pansusceptible | HRZE, C+/SS+ |
| 773 yrs | Female | Italy | Cachexia (BMI<20), vomit and diarrhoea from 8 months, (possible underlying cancer), diabetes mellitus, hypertension, mental disorders | M. tuberculosis new, pulmonary | CT/C-X ray: bilateral excavated lung thickening, tree in bud (right lung) | Pansusceptible | HRZEAdvanced pulmonary TB, SS− (7 days before death) |
| 870 yrs | Male | Spain | Diabetes mellitus, hypertension, obstructive sleep apnea syndrome, renal failure, smoke | M. tuberculosis new, pulmonary | CT/C-X ray: bilateral infiltrates | Pending | HRZE, C pending/SS+ |
BAL: broncho-alveolar lavage; BMI: body mass index; COPD: chronic obstructive pulmonary disease; COVID-19: COronaVIrus Disease 19; CT: computed tomography; EP: extrapulmonary; HBV/HDV: chronic hepatitis B virus and hepatitis delta virus co-infection; HIV: human immunodeficiency virus; HRZE: isoniazid, rifampicin, pyrazinamide, ethambutol; NHL: non-Hodgkin lymphoma; P: pulmonary; SS/C: sputum smear/culture; TB: tuberculosis; TURP: transurethral resection of the prostate.
Continuous variables, if not otherwise specified, are presented as medians (IQR-Interquartile ranges). Categorical variables were described with absolute and relative (percentage) frequencies. Chi-squared and Fisher exact tests were used to compare qualitative variables when appropriate. A two-tailed p-value less than 0.05 was considered statistically significant.
The MuLBSTA (multilobular infiltration, hypo-lymphocytosis, bacterial coinfection, smoking history, hypertension, and age) clinical score used to predict 90- day mortality due to viral pneumonia, although not yet validated for COVID-19, was calculated.10
ResultsOverall, 8 out of 69 (11.6%, 10.6%) patients died, 7 from cohort A (14.3%, patients 1–6.8) and one from cohort B (5%, patient 7) (Tables 1 and 2).
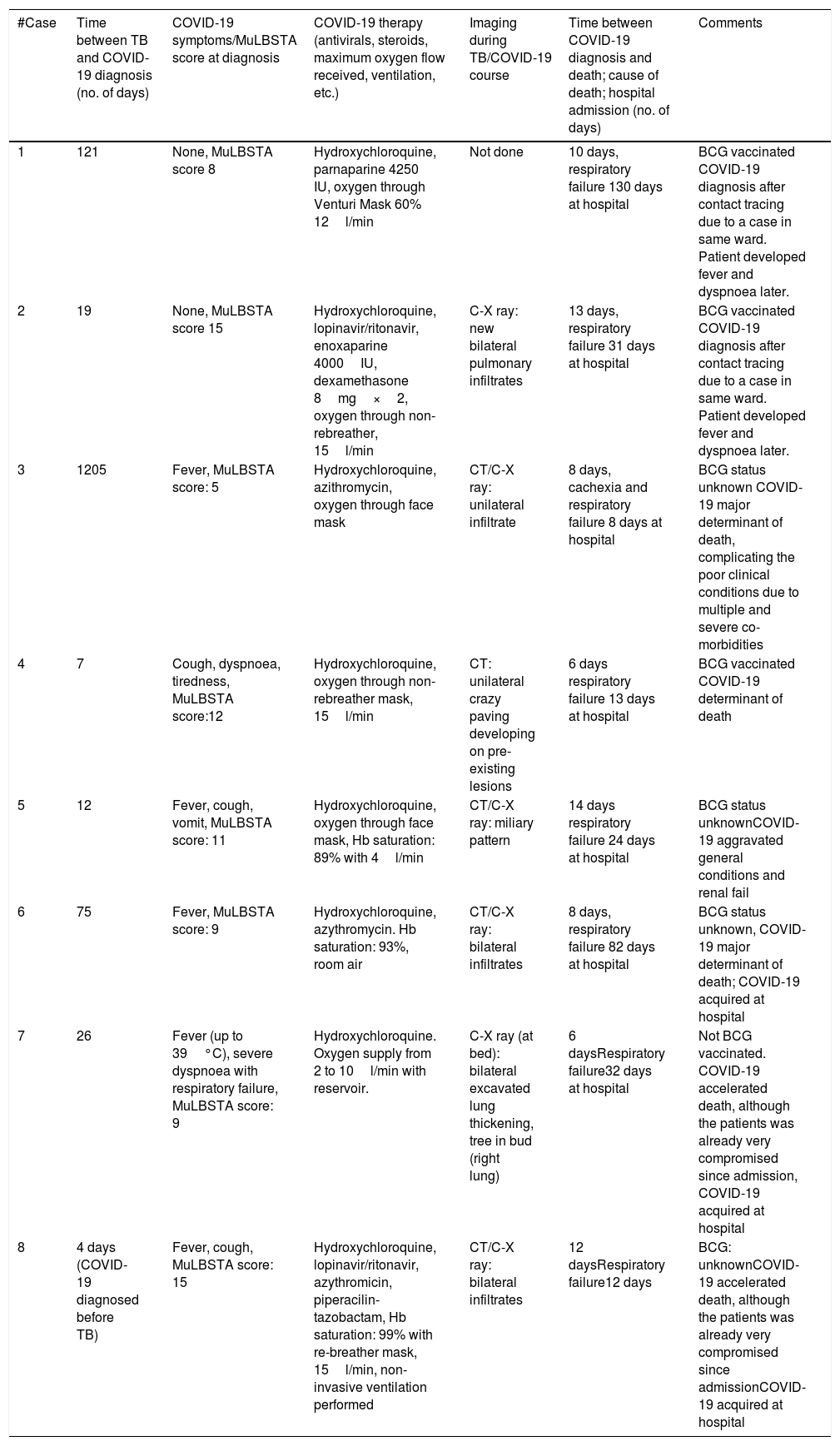
Information on tuberculosis and COVID-19 in 8 patients who died.
| #Case | Time between TB and COVID-19 diagnosis (no. of days) | COVID-19 symptoms/MuLBSTA score at diagnosis | COVID-19 therapy (antivirals, steroids, maximum oxygen flow received, ventilation, etc.) | Imaging during TB/COVID-19 course | Time between COVID-19 diagnosis and death; cause of death; hospital admission (no. of days) | Comments |
|---|---|---|---|---|---|---|
| 1 | 121 | None, MuLBSTA score 8 | Hydroxychloroquine, parnaparine 4250 IU, oxygen through Venturi Mask 60% 12l/min | Not done | 10 days, respiratory failure 130 days at hospital | BCG vaccinated COVID-19 diagnosis after contact tracing due to a case in same ward. Patient developed fever and dyspnoea later. |
| 2 | 19 | None, MuLBSTA score 15 | Hydroxychloroquine, lopinavir/ritonavir, enoxaparine 4000IU, dexamethasone 8mg×2, oxygen through non-rebreather, 15l/min | C-X ray: new bilateral pulmonary infiltrates | 13 days, respiratory failure 31 days at hospital | BCG vaccinated COVID-19 diagnosis after contact tracing due to a case in same ward. Patient developed fever and dyspnoea later. |
| 3 | 1205 | Fever, MuLBSTA score: 5 | Hydroxychloroquine, azithromycin, oxygen through face mask | CT/C-X ray: unilateral infiltrate | 8 days, cachexia and respiratory failure 8 days at hospital | BCG status unknown COVID-19 major determinant of death, complicating the poor clinical conditions due to multiple and severe co-morbidities |
| 4 | 7 | Cough, dyspnoea, tiredness, MuLBSTA score:12 | Hydroxychloroquine, oxygen through non-rebreather mask, 15l/min | CT: unilateral crazy paving developing on pre-existing lesions | 6 days respiratory failure 13 days at hospital | BCG vaccinated COVID-19 determinant of death |
| 5 | 12 | Fever, cough, vomit, MuLBSTA score: 11 | Hydroxychloroquine, oxygen through face mask, Hb saturation: 89% with 4l/min | CT/C-X ray: miliary pattern | 14 days respiratory failure 24 days at hospital | BCG status unknownCOVID-19 aggravated general conditions and renal fail |
| 6 | 75 | Fever, MuLBSTA score: 9 | Hydroxychloroquine, azythromycin. Hb saturation: 93%, room air | CT/C-X ray: bilateral infiltrates | 8 days, respiratory failure 82 days at hospital | BCG status unknown, COVID-19 major determinant of death; COVID-19 acquired at hospital |
| 7 | 26 | Fever (up to 39°C), severe dyspnoea with respiratory failure, MuLBSTA score: 9 | Hydroxychloroquine. Oxygen supply from 2 to 10l/min with reservoir. | C-X ray (at bed): bilateral excavated lung thickening, tree in bud (right lung) | 6 daysRespiratory failure32 days at hospital | Not BCG vaccinated. COVID-19 accelerated death, although the patients was already very compromised since admission, COVID-19 acquired at hospital |
| 8 | 4 days (COVID-19 diagnosed before TB) | Fever, cough, MuLBSTA score: 15 | Hydroxychloroquine, lopinavir/ritonavir, azythromicin, piperacilin-tazobactam, Hb saturation: 99% with re-breather mask, 15l/min, non-invasive ventilation performed | CT/C-X ray: bilateral infiltrates | 12 daysRespiratory failure12 days | BCG: unknownCOVID-19 accelerated death, although the patients was already very compromised since admissionCOVID-19 acquired at hospital |
BCG: Bacillus Calmette-Guérin; COVID-19: COronaVIrus Disease 19; CT: computed tomography; C-X ray: chest radiography; Hb: hemoglobine; IU: international unit; MuLBSTA: multilobular infiltration, hypo-lymphocytosis, bacterial coinfection, smoking history, hyper-tension and age; TB: tuberculosis.
All but one (patient 7) were males, with a median age of 70 (range 45–82) years, and had TB diagnosed before COVID-19; only patient 8 had almost simultaneous diagnosis of COVID-19 and TB. They showed from 2 to 5 co-morbidities, for two patients being cancer (haematological and prostatic, and for patient 7 underlying cancer could not be excluded, although the rapid decline and death prevented the possibility of diagnosing it); one patient was co-infected with HIV and HBV/HDV (chronic hepatitis B virus and hepatitis delta virus).
Out of 69 patients 43 were migrants, 26/49 (53.1%) in cohort A and 17/20 (85.0%) in cohort B.
Migrants were younger than natives: in cohort A the median (IQR) age was 40 (27–49) VS. 66 (46–70) years, whereas in cohort B 37 (27–46) VS. 48 (47–60) years.
Overall, migrants had a lower mortality rate than natives (1/43, 2.3% versus 7/26, 26.9%; p-value: 0.002).
Migrants had fewer co-morbidities than natives; in particular, 23/43 (53.5%) migrants had no co-morbidities versus 5/26 (19.2%) natives (p-value: 0.005).
Among the patients who died, 3 were vaccinated with Bacillus Calmette-Guérin (BCG); 4 were infected by pan-susceptible Mycobacterium tuberculosis strains and one by Mycobacterium bovis, which is intrinsically resistant to pyrazinamide. Except patient 3 who had TB diagnosed in 2016 and was declared cured (affected by post-treatment sequelae) and patient 8 (simultaneous diagnosis of COVID-19 and TB), the remaining patients had COVID-19 diagnosed between 7 and 75 days (median: 22.5 days) after the TB diagnosis. In 6/7 patients SARS-CoV-2 infection was nosocomial.
While only a single patient (patient 3) had unilateral infiltrates, all the others had bilateral lesions: patients 2 and 5 a miliary pattern, patient 4 crazy paving, and patient 7 a ‘tree in bud’ pattern (Tables 1 and 2). TB was treated using first-line drugs; five patients were treated with hydroxychloroquine for COVID-19. Four patients needed oxygen therapy through face mask and one underwent non-invasive ventilation. Death occurred after a median of 9 (range 6–14) days after COVID-19 diagnosis. COVID-19 was considered relevant in either causing death or accelerating its occurrence. Median (range) hospital stay was 27.5 (8–130) days.
The median MuLBSTA score found was 10 (range 8–15) with a theoretical predictive 90-day mortality of 9.33%.
DiscussionTo the best of our knowledge this is the first report of patients dying with TB and COVID-19, including 69 patients from the two largest cohorts of co-infected patients available so far.
Although the case-fatality rate was rather high (overall 10.6%, but 14.3% in the first cohort) and still preliminary (it can increase over time within both cohorts), the results seem consistent with those observed in other cohorts of COVID-19 patients.1–3 In general, all patients (except one) were aged >65 years, and were affected by >2 co-morbidities.
In all cases COVID-19 contributed to worsen the prognosis of TB patients and/or to cause death.
In the majority of patients who died, SARS-CoV-2 infection was nosocomial during early phases of the outbreak in Northern Italy and Spain. This highlights the importance of implementing strict infection control interventions for all hospitalised patients (and, particularly, for those at higher risk, e.g. elderly and patients with co-morbidities including TB), taking into account the risk of viral transmission from other patients, visitors, and healthcare workers.4,5
The MuLBSTA score has been developed for viral pneumonia11 and has similar inputs to risk factors for mortality seen in the initial COVID-19 patient cohorts in China.12 Age has a much stronger odds ratio for increasing mortality in COVID-19 patients than in other viral pneumonia patients. A score higher than 12 points is considered high risk (bacterial coinfection detected by sputum or culture - as for concomitant active TB counts 4 points.) In our patients it does not seem to predict mortality well: the median value is 10 and only 2 patients scored values higher than 12.
TB and COVID-19 seem to absorb relevant human and economic resources, although the relatively small size of the cohort prevents drawing specific conclusions.
The main limitation of this preliminary study is that the cohort, although likely to report the vast majority of cases with TB and COVID-19 in the countries surveyed, cannot be considered representative either of the European nor of the global situation.
The study findings show that: (1) mortality is likely to occur in elderly patients with co-morbidities; (2) TB might not be a major determinant of mortality and (3) migrants had lower mortality, probably because of their younger age and lower number of co-morbidities. However, in settings where advanced forms of TB frequently occur and are caused by drug-resistant strains of M. tuberculosis, higher mortality rates can be expected in young individuals.
However, as the study will continue prospectively with the inclusion of GTN countries where TB and COVID-19 patients have not been diagnosed until now, we wish to invite all interested clinicians and programmes to contact us and participate in the study.
Funding sourceThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interestThe authors have no conflicts of interest to declare.
The article is part of the scientific activities of the Global Tuberculosis Network (GTN); GREPI (Groupe de Recherche et d’Enseignement en Pneumo-Infectiologie), a working group from SPLF (Société de Pneumologie de Langue Française); SEPAR (Sociedad Española de Neumología and Cirugía Torácica); Moscow Society of Phtisiology and of the WHO Collaborating Centre for Tuberculosis and Lung Diseases, Tradate, ITA-80, 2017–2020-GBM/RC/LDA).
The following clinicians participate in the project:
Luigi Ruffo Codecasa (Italy), François-Xavier Blanc (France), Sergey Borisov (Russia), Jan-Willem Alffenaar (Australia), Claire Andréjak (France), Pierre Bachez (Belgium), Pierre-Alexandre Bart (Switzerland), Evgeny Belilovski (Russia), José Cardoso-Landivar (Spain), María-Luiza De Souza-Galvão (Spain), Angel Dominguez-Castellano (Spain), Samir Dourmane (France), Mathilde Fréchet Jachym (France), Antoine Froissart (France), Vania Giacomet (Italy), Soazic Grard (France), Armine Izadifar (France), Damien Le Du (France), Margarita Marín Royo (Spain), Jesica Mazza-Stalder (Switzerland), Maria Musso (Italy), Catherine Wei Min Ong (Singapore), Frédéric Rivière (France), Teresa Rodrigo (Spain), Denise Rossato Silva (Brazil), Matteo Saporiti (Italy), Paolo Scarpellini (Italy), Frédéric Schlemmer (France), Elena Sumarokova (Russia), Paul Anantharajah Tambyah (Singapore), Simon Tiberi (United Kingdom), Alessandro Torre (Italy), Miguel Zabaleta Murguiondo (Spain).


