


Nontuberculous mycobacteria (NTM) are increasingly recognized as causative agents of opportunistic infections in humans for which effective treatment is challenging. There is, however, very little information on the prevalence of NTM drug resistance in Portugal.
Objective and DesignOur aim was to analyze the drug susceptibility testing (DST) performed in NTM at the Portuguese National Health Institute Dr. Ricardo Jorge from February 2003 to February 2016. A total of 262 DST were included in the analysis.
ResultsMost (94%) M. avium intracellulare complex isolates showed in vitro susceptibility to clarithromycin. All M. kansasii isolates were susceptible to rifampicin and ethambutol and 97.1% were susceptible to isoniazid. The majority of rapidly-growing mycobacteria (RGM) demonstrated in vitro susceptibility to amikacin, clarithromycin and cefoxitin. However, in RGM there was a marked increase on the relative risk of having sulfamethoxazole resistance in isolates resistant to ciprofloxacin compared to susceptible isolates.
ConclusionTested NTM in Portugal revealed in vitro susceptibility to most of the antimicrobials currently recommended for treatment. However, our results also suggest that sulfamethoxazole should be avoided in treatment of RGM resistant to ciprofloxacin (or vice versa). Further trials that correlate the in vitro DST results with the clinical outcome are needed in order to reach conclusions on efficient antimicrobial therapy.
Nontuberculous mycobacteria (NTM) are ubiquitous and increasingly recognized as causative agents of opportunistic infections in humans. There are currently over 160 identified species and at least 15 have been considered pathogenic.1 Pulmonary involvement is most frequent, particularly with Mycobacterium avium intracellulare complex (MAC), Mycobacterium kansasii and Mycobacterium abscessus,2–6 and tends to occur in patients with systemic or local immunosuppression such as those infected with HIV or with chronic structural lung disease.2,3,7 NTM acquisition from the environment can occur via inhalation, ingestion or direct inoculation2,3 and, recently, the occurrence of Mycobacterium abscessus complex subsp. massiliense transmissibility between human patients with cystic fibrosis (CF) was suggested by genome sequencing demonstrating the phylogenetic relationship between isolates.8,9
Treatment involves a macrolide-based regimen that differs between species, particularly between rapidly (RGM) and slowly-growing mycobacteria (SGM). The majority of clinical recommendations are, however, based on empirical experience with a relatively few species such as MAC and M. abscessus.2–4 Effective treatment is challenging, probably due to high levels of natural antibiotic resistance,2,3,7 including to many first and second line antibacillary drugs used to treat tuberculosis (TB), which is a main differential diagnosis in NTM lung disease.
Moreover, there seems to be a discrepancy between in vitro antibiotic resistance and the clinical benefit of treatment, particularly in lung disease. These discrepancies derive, in part, from laboratory technical difficulties of drug susceptibility testing (DST), absence of standardized methods and lack of clinical validation.7 However, the mechanisms involved are poorly understood and findings suggest that more than just antibiotic resistance is involved.4,7,10 For instance, it has been shown that M. abscessus is capable of structured cord formation, a biofilm mode of growth, in explanted lungs of CF patients, and suggested that antibiotic resistance could be inferred by this protective coat.10–12 Demonstrating NTM biofilm growth in the human lung could improve treatment options as well as laboratory techniques used in DST.10 Some molecular methods (such as sequencing of 16S rRNA and 23S rRNA genes) could also help assess drug susceptibility, but are not yet routinely available.9 The discrepancy between laboratory findings and clinical outcome tends to be less evident in nonpulmonary disease. In fact, treatment of RGM nonpulmonary disease is currently based on in vitro susceptibilities.2
Recommended drugs for DST in SGM include: (1) clarithromycin in previously untreated MAC isolates; (2) clarithromycin, moxifloxacin and linezolid in MAC from patients who fail macrolide treatment or prophylaxis regimens; (3) rifampicin and, more recently, clarithromycin10,13 in previously untreated M. kansasii isolates; and (4) rifabutin, ethambutol, isoniazid, clarithromycin, fluoroquinolones, amikacin, sulfonamides and linezolid in M. kansasii resistant to rifampicin.2,10 Recommended DST in RGM include amikacin, cefoxitin, ciprofloxacin, clarithromycin, doxycycline-minocycline, imipenem-meropenem, linezolid, moxifloxacin, tobramycin, and trimethoprim-sulfamethoxazole.2,10,13
In Portugal, all NTM DST are performed at the Portuguese National Health Institute according to the above mentioned recommendations and at clinician request. Although the role of DST in the choice of agents for antimicrobial treatment of NTM disease is still debatable, with the increased clinical importance of NTM disease, DST may be again in the spotlight.7
ObjectiveTo describe the in vitro resistance patterns to antibiotics of the NTM sent to DST in Portugal.
Material and methodsDatabase designResults of the NTM DST performed from February 2003 to February 2016 at the Portuguese National Health Institute were collected. Information on species level, antibiotic susceptibility, district of isolation, previous known isolation of NTM sent to DST, and specimen used, was included in a database for analysis. The DST were performed according to the broth microdilution method and the resistance criteria described in the National Committee for Clinical Laboratory Standards (NCCLS) from 2003 to 201114 and in the Clinical and Laboratorial Standards Institute (CLSI) after 2011.13
Statistical analysisMicrosoft EXCEL (2013) and SPSS (version 24.0) were the data analysis tools used. As all considered variables were nominal with several categories, descriptive statistics consisted of number of cases (counts and/or proportions/percentages) that were structured in frequency tables of one variable and cross frequency tables of two variables. Contingency tables were produced to compare the homogeneity of the resistance response to one given antibiotic of certain categories of RGM from two subpopulations. The chi-square test of homogeneity was carried out to test the null hypothesis that resistance responses were identical in two subpopulations. The comparison of the two proportions (assuming binary attributes) was performed by using the two proportions z-test.15 The level of significance was set at a p<0.05.
ResultsA total of 262 DST were included, which were performed in: 153 MAC, 36 M. kansasii, 32 M. abscessus, 22 M. chelonae, 11 M. fortuitum, 1 M. peregrinum, 1 M. mucogenicum and 6 less frequent NTM – M. marinum, M. triplex, M. scrofulaceum, M. gordonae, M. szulgai and M. malmoense.
Mycobacterium avium intracellulare complexFifty-three (34.6%) isolates were from the district of Porto and 31 (20.3%) from Lisbon (Supplemental Material, Figure S1). It was not possible to retrieve information about isolation district of 2 samples. All MAC isolates were tested for clarithromycin and 94% revealed in vitro susceptibility. Of the 9 macrolide-resistant isolates, 4 were from Porto, 4 from Lisbon and 1 from Viana do Castelo. There was no significant difference between the proportions of clarithromycin-resistant isolates for Lisbon and Porto districts (p=0.4197, z-test). Fifty-six (36.6%) isolates were from patients who had already had one known MAC isolate sent to DST in the past, including 7 clarithromycin-resistant isolates. In 85 (56%) samples, the specimen used for DST was specified and included a total of 74 (87%) respiratory specimens: 46 (54%) sputum, 27 (32%) bronchial secretions and 1 lung biopsy.
Mycobacterium kansasiiHalf (52.8%) of the isolates were from the district of Porto and 27.8% from Lisbon. All M. kansasii showed in vitro susceptibility to rifampicin. Thirty-five (97.2%) isolates were tested with isoniazid and ethambutol and 97.1% showed isoniazid susceptibility while all of them were susceptible to ethambutol. Only 4 of the samples were from patients who had had a previous M. kansasii isolate sent to DST. Of the 20 (55.6%) samples with information regarding the specimen used for DST, 95% were from the respiratory tract, either sputum (85%) or bronchial secretions (10%).
Rapidly-growing mycobacteria (RGM)A total of 67 RGM DST were analyzed. Almost half (43.3%) of the isolates were from the district of Lisbon and 23.9% from Porto (Figure S2). It was not possible to retrieve information about isolation district for 3 samples.
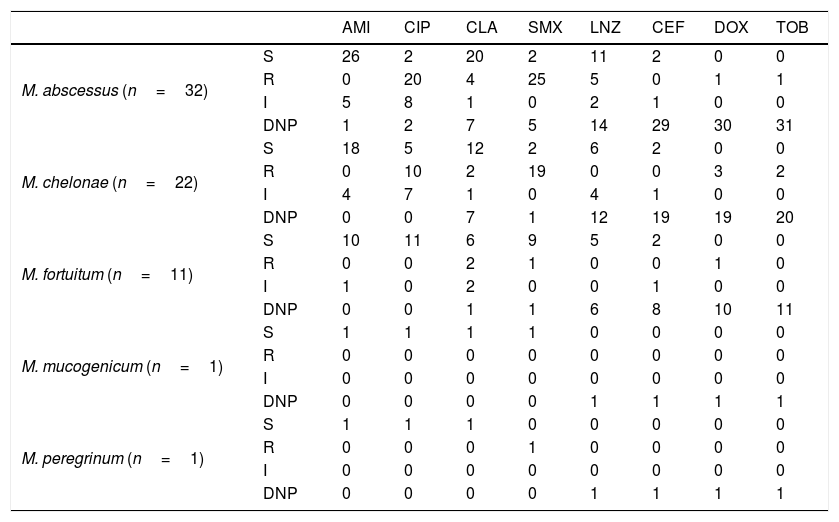
Results of the RGM DST are shown in Table 1 and further specified in Table S1.
Patterns of resistance to antibiotics of the RGM sent to DST during February 2003 to February 2016.
| AMI | CIP | CLA | SMX | LNZ | CEF | DOX | TOB | ||
|---|---|---|---|---|---|---|---|---|---|
| M. abscessus (n=32) | S | 26 | 2 | 20 | 2 | 11 | 2 | 0 | 0 |
| R | 0 | 20 | 4 | 25 | 5 | 0 | 1 | 1 | |
| I | 5 | 8 | 1 | 0 | 2 | 1 | 0 | 0 | |
| DNP | 1 | 2 | 7 | 5 | 14 | 29 | 30 | 31 | |
| M. chelonae (n=22) | S | 18 | 5 | 12 | 2 | 6 | 2 | 0 | 0 |
| R | 0 | 10 | 2 | 19 | 0 | 0 | 3 | 2 | |
| I | 4 | 7 | 1 | 0 | 4 | 1 | 0 | 0 | |
| DNP | 0 | 0 | 7 | 1 | 12 | 19 | 19 | 20 | |
| M. fortuitum (n=11) | S | 10 | 11 | 6 | 9 | 5 | 2 | 0 | 0 |
| R | 0 | 0 | 2 | 1 | 0 | 0 | 1 | 0 | |
| I | 1 | 0 | 2 | 0 | 0 | 1 | 0 | 0 | |
| DNP | 0 | 0 | 1 | 1 | 6 | 8 | 10 | 11 | |
| M. mucogenicum (n=1) | S | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 |
| R | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| I | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| DNP | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | |
| M. peregrinum (n=1) | S | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 |
| R | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | |
| I | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| DNP | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 |
S, Susceptibility; R, Resistance; I, Intermediate resistance; DNP, DST not performed; AMI, Amikacin; CIP, Ciprofloxacin; CLA, Clarithromycin; SMX, Sulfamethoxazole; CEF, Cefoxitin; DOX, Doxycycline; TOB, Tobramycin; LNZ, Linezolid.
In RGM, levels of resistance to ciprofloxacin and sulfamethoxazole were high. The relative risk of having sulfamethoxazole resistance was 2.6 times higher in isolates resistant (including intermediate resistant) to ciprofloxacin compared to susceptible isolates. Resistance to sulfamethoxazole was strongly associated with resistance to ciprofloxacin (z-test, p<0.001) (Fig. 1, Table S2).
 and sulfamethoxazole (SXT) in RGM suggest a strong correlation on the relative risk of having sulfamethoxazole resistance in isolates resistant to ciprofloxacin compared to susceptible isolates. In the fraction of the population with RGM CIP Susceptible only 37% of the individuals displayed resistance to SXT. However, in the fraction of population with RGM CIP Resistant alone (R) or combined with Intermediate resistance (R+I), 100% or 95% of the individuals also displayed resistance to SXT, respectively (*** stands for p<0.001, z-test; R, resistant; I, intermediate resistant).")
Relative risk of cross resistance in RGM. Cross-susceptibility profiles to ciprofloxacin (CIP) and sulfamethoxazole (SXT) in RGM suggest a strong correlation on the relative risk of having sulfamethoxazole resistance in isolates resistant to ciprofloxacin compared to susceptible isolates. In the fraction of the population with RGM CIP Susceptible only 37% of the individuals displayed resistance to SXT. However, in the fraction of population with RGM CIP Resistant alone (R) or combined with Intermediate resistance (R+I), 100% or 95% of the individuals also displayed resistance to SXT, respectively (*** stands for p<0.001, z-test; R, resistant; I, intermediate resistant).
There was no statistically significant heterogeneity (chi-square test, p=0.788) between specimens from Porto and Lisbon regarding resistance to ciprofloxacin and sulfamethoxazole both in M. abscessus and M. chelonae (Tables S3 and S4). Twelve (17.9%) samples, including 9 M. abscessus, 2 M. chelonae and 1 M. fortuitum, were from patients with a previous RGM isolate sent to DST. Three of these M. abscessus and both M. chelonae isolates were resistant to clarithromycin.
DiscussionNTM species found in DST from PortugalAt present there are not many studies addressing NTM antibiotic resistance patterns.16,17 A study in Beijing found high levels of resistance to first and second line anti-tuberculous drugs. However, they did not include macrolides in the analysis.16 Our retrospective study included 262 NTM DST, which were requested according to clinician criteria and sent to the national reference center in Portugal. The majority of the isolates were from respiratory specimens. MAC was the most frequently tested species (58.4%). Accordingly, in a recent epidemiology survey,17 MAC was the most frequently isolated species in NTM-Pulmonary Disease (NTM-PD) in Europe, with proportions of 44.8% in Lisbon, Portugal, between 2008 and 2009. NTM-PD due to M. kansasii has been more frequent in Europe than in North America, particularly in London, where it was the most frequently isolated species between 2000 and 2007.17 In our study, M. kansasii was the second most frequently tested species (13.7%). In North America, M. abscessus and M. chelonae are frequent in NTM-PD after MAC while in Europe percentages have been more variable.17 In this study, 67 RGM were analyzed, including 32 M. abscessus (12.2% of all NTM) and 22 M. chelonae (8.4%).
Antibiotic resistance in NTMGlobally, tested NTM exhibited in vitro susceptibility to most of the antibiotics currently recommended for treatment. Susceptibility profiles to antimicrobials were identical in the two main Portuguese districts – Lisbon and Porto. However, based on current published data, the exact role of DST and its potential to guide regimen selection and predict outcomes in NTM-PD remains unknown. It is important to appreciate that, although CLSI guidelines provide breakpoint concentrations to interpret minimum inhibitory concentrations (MICs) as ‘susceptible’ or ‘resistant’, these cut-offs have had very limited clinical validation.9
In this study, most MAC exhibited in vitro susceptibility to clarithromycin which is the mainstay recommended antibiotic for clarithromycin sensitive MAC-PD.2,3,9,18 Although it was not possible to retrieve information about the specimen used for DST in 44.4% of the samples it should be noted that from the remainder, 87% were from respiratory specimens. Ethambutol, rifampin and aminoglycosides, which are also recommended for treatment, were not used in the samples since there are no clinical recommendations for DST with these drugs in MAC. In this study, only 6% of the isolates were resistant to clarithromycin which predicts worse clinical outcomes and requires augmented treatment. Major risk factors for the development of clarithromycin-resistant MAC are macrolide monotherapy and prior macrolide treatment with inadequate companion medications.9 Thus, it should be noted that of the 9 clarithromycin-resistant isolates, 7 were from patients for whom a previous MAC isolate had been sent to DST, most likely reflecting isolates already subject to antibiotic pressure. The relative risk of having clarithromycin resistance was 6 times higher in isolates from patients who had had previous isolates sent to DST (z-test, p<0.01) (Table S5).
All M. kansasii had in vitro susceptibility to rifampicin, which is the recommended antimicrobial for DST and treatment.2,3,18 All isolates also revealed susceptibility to ethambutol and 97.1% to isoniazid, which are included in the recommended first-line antimicrobial regimen. The role of DST for these two antimicrobials is, however, debatable and testing and interpretation of isoniazid results may be technically difficult.10
Most RGM demonstrated in vitro susceptibility to macrolides which are the recommended mainstay antibiotics for treatment,2,3,18 and the only oral drugs with consistent in vitro activity.9 However in series of M. abscessus-PD, outcomes of macrolide-based treatment are generally poor and do not correlate well with in vitro susceptibilities, potentially due to erm41-dependent inducible macrolide resistance, acquired point mutations in the 23S-rRNA and relatively short duration of adequate regimens, often interrupted due to toxicity.9 In this study it was possible to retrieve information regarding specimen origin in 13 (40.6%) M. abscessus and all were from the respiratory tract, which might limit the clinical meaning of the DST results.
For RGM, clinical validation of DST has only been performed in series of extrapulmonary disease, and only for aminoglycosides, sulfamethoxazole and cefoxitin.9 In this study 85% of the RGM were susceptible to amikacin and 67% to cefoxitin, suggesting that these might be good candidates for treatment while sulfamethoxazole might be of little benefit, since 77% of the isolates were resistant to this antibiotic. However, although it was not possible to retrieve information regarding the specimen used for DST in many RGM (67%), it should be noted that where it was possible all were from respiratory specimens, which may once again limit the clinical validation of the results.
Linezolid shows in vitro activity in approximately 50% of M. abscessus isolates (although there is considerable geographical variation).9 In this study 33 RGM (including 18 M. abscessus) were tested with linezolid and 67% were susceptible. It should be noted, however, that in clinical practice hematological and neurological toxicities are common, particularly with prolonged courses and that care should be exercised in individuals chronically co-infected with methicillin-resistant Staphylococcus aureus (MRSA) since long-term linezolid therapy may encourage MRSA resistance.9
Fluoroquinolones and doxycycline rarely show in vitro activity in RGM.9 Accordingly, 65 RGM were tested with ciprofloxacin and many (46%) were resistant while of the six RGM tested with doxycycline only one was susceptible to this antibiotic.
Relative risk of cross resistance in NTMAlarmingly, in RGM there was a strong correlation on the relative risk of sulfamethoxazole resistance in isolates resistant to ciprofloxacin compared to susceptible isolates. Interestingly, a recent review of global fluoroquinolone resistance rates reports a much higher odds ratio for fluoroquinolone resistance in multi-drug resistant (MDR)-TB compared to non-MDR-TB.19 This is consistent with our observation. At this moment in time it is difficult to speculate about the molecular mechanism giving rise to this pattern, particularly since mycobacteria have several poorly studied intrinsic and acquired mechanisms of drug resistance.20 Both ciprofloxacin and sulfamethoxazole target essential cellular functions, thus the evolutionary acquisition of resistance – especially by the acquisition of chromosomal mutations – is usually associated to a detrimental effect in the absence of the drug.21 However, there are exceptions to this “rule” and it is known that some microorganisms have the ability to acquire resistance to ciprofloxacin at low cost which can be quickly compensated.22,23 The frequent occurrence of ciprofloxacin and sulfamethoxazole resistance in RGM even in the absence of a previously isolated RGM sent to DST should also take into consideration the fact that this disease more frequently occurs in patients who are highly likely to have had previous antibiotic therapy or prophylaxis with these drugs (e.g. cystic fibrosis and HIV infection).
Limitations of the studyOne limitation of this study was the inability to reliably cross microbiological information with clinical variables such as NTM disease criteria, antibiotic regimens and course of the disease. Data was limited to the information contained in the hand-written DST records available at the Portuguese National Health Institute, which did not contain enough data to retrospectively match samples with patients. Secondly, the available database has some bias due to heterogeneity of antibiotics tested in RGM. However, DST were performed according to the current recommendations as well as the clinician request which took into consideration the clinical variables (co-morbidities, allergies and patient's preference or compliance to oral or injectable medication) as well as the empiric antibiotic regimen instituted.
Data relating to specimens used for DST and previous isolates of NTM in the same patient was limited. Previous isolates were defined as DST records from the same patient at least one month apart from each other, which could represent the same NTM specimen and in some cases circumstances of unresponsiveness to treatment or retreatment. However many DST were also performed in previously untreated NTM, according to recommendations. Only NTM sent to DST were tested, which constitute a confined proportion of the global NTM isolates, but should reflect the isolates with clinical relevance. Despite the pitfalls of DST for NTM, our results for frequent ciprofloxacin and sulfonamides joined resistance in RGM should be highlighted, since for these strains antibiotic regimens are still primarily based on DST results.2,7 Moreover, as far as we know, this is the first attempt at creating a database on the antibiotic resistance of NTM in Portugal.
ConclusionResults of the NTM DST performed in Portugal favor most current treatment recommendations. However, their clinical meaning was not assessed. Since ciprofloxacin-resistant RGM isolates have a higher risk of also being resistant to sulfamethoxazole, our study suggests that sulfamethoxazole should be avoided when treating RGM resistant to ciprofloxacin, and vice versa. However, further studies are needed to corroborate the generalization of this finding and to reach conclusions on efficient antimicrobial therapy.
Author contributionsAll authors conducted the literature review. RD and VD conceptualized the study. AS and RM performed the NTM species identification and DST. VD collected the data. VD and PD conducted the analyses. All authors interpreted and discussed the results. VD wrote the manuscript. All authors have read and approved the final version.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank Fernando Durão PhD (Instituto Superior Técnico de Lisboa, Lisbon, Portugal), for his contribution to the statistical analysis. The authors would also like to thank the Portuguese National Health Institute Dr. Ricardo Jorge for providing access to the DST results.


